Iron-Rich Foods for Pregnancy: Safe Sources for Mom and Baby
Iron deficiency affects 40% of pregnant women worldwide. Fetal brain development depends on it. 15 safe iron-rich foods, the vitamin C absorption rule, foods to avoid.
by BiteBrightly
3/22/202628 min read
Iron-Rich Foods for Pregnancy: Safe Sources for Mom and Baby
By BiteBrightly 22 March 2026: This post might contain affiliate links.
Pregnancy changes your relationship with food in ways that go far beyond cravings and aversions. The nutritional demands of growing a human being are specific, urgent, and in some cases dramatically higher than anything your body has previously required. Iron is perhaps the clearest example of this. Before pregnancy, a woman needs 18mg of iron daily. During pregnancy, that requirement nearly doubles to 27mg — a 50% increase that most women, regardless of how thoughtfully they ate before conception, are unprepared for and frequently fail to meet.
The consequences of this shortfall are not minor. Iron deficiency anemia in pregnancy — the most common nutritional deficiency globally affecting pregnant women — is associated with premature birth, low birth weight, postpartum depression, impaired infant neurodevelopment, and maternal death in severe cases. The developing brain in particular is profoundly dependent on adequate iron in the second and third trimesters, when iron-dependent enzymes drive the myelination of nerve fibers, the differentiation of dopaminergic neurons, and the energy metabolism of rapidly dividing neural tissue. Iron deficiency during these critical windows produces neurological consequences in the infant that may not become apparent until school age — attention and memory deficits, reduced processing speed, and behavioral difficulties — and that may not be fully correctable by later iron repletion.
This is a nutritional priority that matters enormously, and yet the practical guidance most pregnant women receive is often limited to "take your prenatal vitamin and eat more spinach." Both recommendations are incomplete. Prenatal vitamins vary enormously in their iron content, form, and bioavailability. And spinach — the most commonly cited dietary iron source — is one of the least bioavailable iron foods available, because spinach's high oxalic acid content binds iron in insoluble complexes that cannot be absorbed.
The goal of this guide is to give you the complete, mechanistically accurate picture: what iron does during pregnancy, why the requirement increases so dramatically, the fifteen most iron-rich foods that are both effective and safe in pregnancy, the critical distinction between heme and non-heme iron and the dietary strategies that dramatically improve absorption, the foods and habits that silently block iron absorption, and the practical framework for meeting the 27mg daily target through food and appropriate supplementation.
Key Takeaways
Iron requirements increase from 18mg to 27mg daily during pregnancy — a 50% increase that most women do not meet through diet alone, making iron-rich food choices and often supplementation essential
Iron deficiency is the most common nutritional deficiency in pregnant women globally — affecting approximately 40% of pregnant women worldwide, with serious consequences for both maternal and fetal outcomes
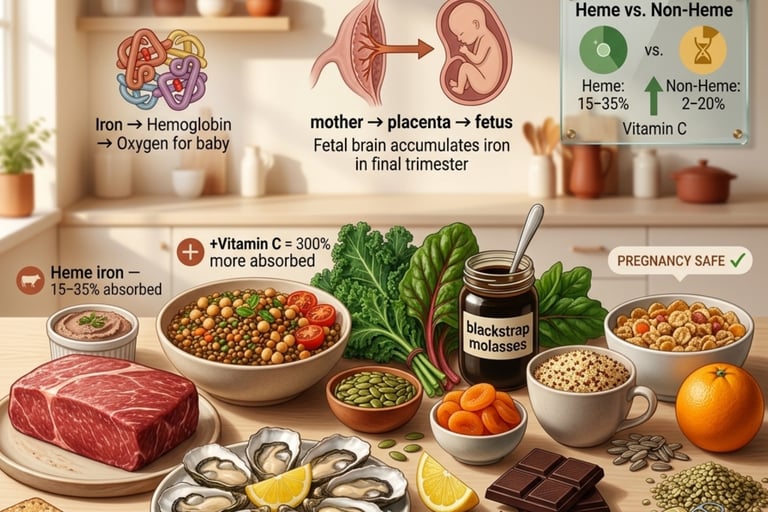
Heme iron (from animal sources — red meat, poultry, fish, organ meats) is absorbed at 15–35% efficiency regardless of other dietary factors; non-heme iron (from plant sources) is absorbed at only 2–20%, but absorption can be dramatically increased by dietary strategies
Vitamin C consumed with non-heme iron increases absorption by up to 300% — the single most important absorption strategy for plant-based iron sources
Calcium, tannins (from tea and coffee), phytates (from whole grains and legumes), and polyphenols block iron absorption — timing iron-rich meals away from dairy, tea, and coffee is as important as eating iron-rich foods
Cooking in cast iron cookware — particularly with acidic foods — adds meaningful dietary iron, with some studies showing 5–7mg of iron added per serving of tomato-based dishes cooked in cast iron
Liver is the most iron-dense food available but requires caution in pregnancy — its extremely high vitamin A (retinol) content at excess doses is teratogenic; consumption should be limited to once per week maximum
The combination of heme iron + non-heme iron at the same meal improves total iron absorption from the non-heme sources — a phenomenon called the "meat factor"
Why Iron Demands Surge in Pregnancy
The Physiology of Pregnancy Iron Demand
The dramatic increase in iron requirement during pregnancy is driven by several simultaneous biological processes, each making significant iron demands on the mother's reserves.
Expanded blood volume: Plasma volume increases by 40–50% during pregnancy — the most dramatic cardiovascular adaptation to pregnancy. Red blood cell mass increases by 20–30% to maintain adequate oxygen-carrying capacity within this expanded plasma. Each new red blood cell contains hemoglobin — and each hemoglobin molecule requires four iron atoms at its core. This expansion in red blood cell mass requires approximately 450–500mg of iron over the course of pregnancy.
Fetal iron accumulation: The developing fetus accumulates iron actively against a concentration gradient — iron in fetal blood reaches concentrations two to three times higher than in maternal blood, reflecting the high-priority biological status of fetal iron storage. The fetus accumulates approximately 270–300mg of iron during pregnancy, most of it in the final trimester when fetal growth is most rapid. This fetal iron comes entirely from the mother — the placenta has no independent iron source.
Placental iron: The placenta itself requires approximately 50–75mg of iron for its own development and function. The placental syncytiotrophoblast cells — the cells that interface with maternal blood — express transferrin receptors that actively capture maternal transferrin-bound iron and transfer it to the fetal circulation, prioritizing the fetus even when maternal iron stores are depleted.
Iron for fetal brain development: The developing brain accounts for a disproportionate share of fetal iron demand. Iron is required for myelination (the process by which nerve fibers acquire the myelin sheath that enables rapid electrical conduction), for the synthesis of monoamine neurotransmitters (dopamine, serotonin, and norepinephrine all require iron-dependent enzymes), and for mitochondrial oxidative phosphorylation in the energy-intensive neural tissue. The hippocampus — the brain region responsible for memory formation and spatial navigation — is particularly vulnerable to iron deficiency, with animal and human research consistently showing hippocampal iron deficiency producing long-lasting memory and learning impairments.
Postpartum losses: Blood loss during delivery — approximately 300–500ml in vaginal delivery and 500–1,000ml in cesarean — represents an additional iron drain that pregnancy iron stores must also partially cover.
The Trimester-by-Trimester Picture
Iron requirements are not uniform throughout pregnancy — they escalate dramatically as pregnancy progresses.
First trimester (weeks 1–13): Iron requirement is actually somewhat lower than pre-pregnancy in many women — approximately 0.8mg/day of absorbed iron. This is because menstruation has ceased (eliminating the monthly 15–20mg iron loss) and fetal demands are modest in early pregnancy. Many women experience first-trimester nausea and food aversions that make iron-rich foods difficult to consume — but the physiological demand at this stage, while real, is less urgent than in later pregnancy.
Second trimester (weeks 14–27): Iron absorption and demand increase significantly. Blood volume expansion accelerates. The fetal nervous system is developing rapidly. Dietary iron intake and absorption strategies become critically important during this window. Women who enter the second trimester with marginal iron stores frequently develop iron deficiency anemia by the third trimester.
Third trimester (weeks 28–40): Iron requirements peak — approximately 6–10mg/day of absorbed iron during the final months, when fetal iron accumulation is most rapid and blood volume expansion is at its greatest. The body adapts by dramatically upregulating intestinal iron absorption — a healthy woman absorbs iron at 3–4 times her pre-pregnancy rate in the third trimester — but this adaptation cannot compensate for poor dietary iron intake or inadequate iron stores entering pregnancy.
Understanding Heme vs. Non-Heme Iron: The Absorption Difference
Before reviewing the fifteen best iron foods for pregnancy, understanding the fundamental distinction between heme and non-heme iron is essential — because these two forms behave completely differently in the digestive system, with bioavailability differences that can make the difference between iron sufficiency and iron deficiency even at the same total iron intake.
Heme iron is derived from the hemoglobin and myoglobin in animal muscle tissue. It is absorbed directly across the intestinal mucosa via a specific heme transporter (HCP1/PCFT), bypassing the competitive regulatory mechanisms that govern non-heme iron absorption. Heme iron is absorbed at approximately 15–35% efficiency and is largely unaffected by the presence of absorption inhibitors (calcium, tannins, phytates, oxalates) in the meal. Sources: red meat, poultry, fish, and organ meats.
Non-heme iron is derived from plant foods, eggs, dairy, and fortified foods. It enters the intestinal enterocyte via the divalent metal transporter DMT-1, which it shares with calcium, zinc, and manganese — meaning these minerals compete for the same absorption pathway. Non-heme iron must first be reduced from the ferric form (Fe³⁺) to the ferrous form (Fe²⁺) by duodenal cytochrome B reductase — a reduction that is facilitated by vitamin C. Non-heme iron absorption ranges from as low as 2% to as high as 20% depending on:
Iron status of the individual (lower iron stores → upregulated DMT-1 → higher absorption efficiency)
Vitamin C content of the meal (ascorbic acid reduces ferric to ferrous iron and prevents the formation of insoluble iron complexes)
Presence of inhibitors (calcium, tannins, phytates, oxalates block DMT-1 absorption)
Presence of the "meat factor" from simultaneously consumed heme iron sources
The practical implication: a pregnant woman eating 15mg of iron from plant sources with poor absorption strategies may absorb as little as 0.3–1.5mg of elemental iron. The same 15mg of iron from plant sources consumed with a vitamin C-rich food, separated from tea, coffee, and dairy, and alongside a small amount of heme iron, may yield 2–3mg of absorbed iron — a six-to-ten-fold difference from the same food at the same total iron intake.
The 15 Best Iron-Rich Foods for Pregnancy
1. Beef and Lamb (Red Meat)
Lean red meat is the most practically significant iron food in pregnancy — providing highly bioavailable heme iron at the highest concentrations available from everyday protein sources, alongside zinc (critical for fetal immune and neurological development), vitamin B12, and the complete amino acid spectrum required for fetal tissue synthesis.
How it works: A 3-ounce serving of lean beef provides approximately 3.2mg of iron — approximately 80% as heme iron — absorbed at 15–35% efficiency regardless of other dietary factors. This means a 3-ounce beef serving reliably delivers 0.5–1.1mg of absorbed iron, making it the highest single-meal absorbed iron contribution of any non-organ meat source.
Beyond iron itself, red meat provides the "meat factor" — an as-yet uncharacterized compound in meat tissue that enhances the absorption of simultaneously consumed non-heme iron by up to 150%. A meal of beef with lentils and spinach will produce significantly more total absorbed iron than the lentils and spinach eaten without the beef, due to this meat factor enhancement of plant iron absorption.
Zinc from red meat (approximately 5.3mg per 3oz beef — 48% of pregnancy zinc requirement) is equally important: zinc deficiency in pregnancy is associated with fetal growth restriction, preterm delivery, and congenital abnormalities, and zinc is a direct cofactor for the enzymes driving fetal DNA synthesis.
Safety note: All red meat must be cooked to an internal temperature of at least 71°C (160°F) during pregnancy — listeria and toxoplasma, both of which pose serious fetal risks, can be present in undercooked red meat. Deli meats, cured meats, and cold cuts should be heated until steaming before consumption.
How to use it: Lean ground beef, sirloin, or lamb 2–4 times weekly — in bolognese sauce with lentils (meat factor enhancing lentil iron absorption), in stir-fries with bell peppers (vitamin C amplifying iron absorption), in soups and stews with legumes, or as a simple pan-cooked protein alongside iron-rich vegetables. Pair with tomatoes, citrus, or bell peppers at the same meal for maximum iron absorption from both the heme and non-heme sources.
2. Chicken Liver
Chicken liver is the most iron-dense food available in the safe pregnancy category — providing 12.8mg of iron per 3-ounce serving (47% of the 27mg daily pregnancy requirement in a single serving) in a form that is almost entirely heme iron with maximum bioavailability.
How it works: Chicken liver provides heme iron at concentrations that no other commonly available food approaches, alongside vitamin B12 (the highest of any food), folate (550mcg per 3oz — critical for neural tube development), zinc, copper, and selenium in comprehensively optimal amounts for fetal development. The iron in liver is stored ferritin iron from the animal's own hepatic iron stores — the most bioavailable form of heme iron available from any food source.
The vitamin A consideration — critical: This is the most important safety note in this entire guide. Beef liver (more than chicken liver) contains extraordinarily high amounts of preformed vitamin A (retinol). Excess preformed vitamin A is teratogenic — it causes fetal malformations, particularly of the heart, brain, and limbs — and the safe upper limit in pregnancy is 3,000mcg RAE (retinol activity equivalents) or approximately 10,000 IU daily. A single serving of beef liver can provide 15,000–30,000 IU of preformed vitamin A — far exceeding safe pregnancy limits. Chicken liver is significantly lower (approximately 4,000–6,000 IU per 3oz serving), making it safer for weekly consumption in pregnancy, but still requiring moderation.
Pregnancy recommendation: Chicken liver once per week provides exceptional iron delivery within safe vitamin A boundaries. Beef liver once per week is borderline acceptable for most women but should be discussed with an obstetrician or midwife. Beef liver more than once weekly during pregnancy is not recommended due to vitamin A teratogenicity risk. Always cook liver until well done — no pink remaining.
How to use it: Chicken liver pâté on whole grain crackers with lemon (vitamin C enhancing further absorption), pan-fried chicken livers with garlic and onion over brown rice, or added to bolognese sauce where the strong liver flavor is masked by the tomato-based preparation. Lemon juice alongside liver not only adds vitamin C for additional non-heme iron enhancement but also helps balance the rich flavor.
3. Oysters (Cooked)
Oysters are the most zinc-dense food available and provide substantial heme iron alongside — but the critical pregnancy caveat is that raw oysters are absolutely contraindicated in pregnancy due to Vibrio bacteria and other foodborne pathogens that pose serious fetal and maternal risk.
How it works: Six medium cooked oysters provide approximately 5.7mg of iron alongside 74mg of zinc (670% of the daily zinc requirement), selenium, vitamin D, and omega-3 fatty acids. The iron is primarily heme iron with the high bioavailability characteristic of shellfish. Oysters' extraordinary zinc density makes them uniquely valuable for pregnancy beyond their iron content — zinc supports fetal immune system development, neural tube closure, and placental function.
Safety: Cooked oysters only — steamed, baked, or in cooked preparations. The Vibrio bacteria that make raw oysters dangerous are destroyed by thorough cooking. Pre-packaged cooked oyster products (smoked oysters in cans) are safe and convenient.
How to use it: Canned smoked oysters on whole grain crackers with lemon juice (iron + vitamin C combination), cooked oysters in soups or chowders, or steamed oysters as an appetizer. Canned oysters are nutritionally comparable to fresh cooked and significantly more convenient — check labels for water-packed varieties to minimize sodium.
4. White Beans and Legumes (Lentils, Chickpeas, Kidney Beans)
Legumes are the most important iron source for pregnant women with plant-forward dietary patterns and a critically important iron contributor for all pregnant women — providing non-heme iron at the highest concentrations of any plant food alongside folate, protein, and fiber.
How it works: One cup of cooked white beans provides 8mg of iron — the highest of any common legume. Lentils provide 6.6mg per cup cooked; kidney beans 5.2mg; chickpeas 4.7mg. These are substantial amounts of non-heme iron, and the key to realizing their full potential is optimizing absorption through vitamin C pairing and inhibitor avoidance.
Legumes are also the richest plant source of folate — a nutrient whose critical importance in preventing neural tube defects makes it the most universally supplemented nutrient in pregnancy. One cup of lentils provides 358mcg of folate — nearly the entire 400mcg recommended for fetal neural tube protection. The iron + folate combination in legumes makes them uniquely comprehensive for pregnancy nutrition.
The phytate content of legumes (a primary non-heme iron absorption inhibitor) can be substantially reduced by soaking dried legumes for 12–24 hours before cooking — reducing phytate content by 30–50% and meaningfully improving iron (and zinc) bioavailability. Canned legumes, which have been extensively processed, have significantly reduced phytate compared to dry beans and can be used as a higher-bioavailability convenience option.
How to use it: Lentil soup with tomatoes and lemon (non-heme iron + vitamin C from both tomatoes and lemon); white bean and kale stew with a squeeze of lemon; chickpea curry with tomatoes and bell peppers; hummus with red bell pepper crudités (vitamin C from peppers dramatically enhancing chickpea iron absorption). Always include a vitamin C source in the same meal and avoid consuming tea, coffee, or dairy at the same time.
5. Dark Leafy Greens (Spinach, Kale, Swiss Chard, Collard Greens)
Dark leafy greens provide non-heme iron alongside folate, calcium, vitamin C (particularly kale and broccoli), and beta-carotene — but with an important nuance that changes their practical iron value significantly depending on the specific green chosen.
How it works: One cup of cooked spinach provides 6.4mg of iron — impressive on paper, but spinach also contains approximately 975mg of oxalic acid per 100g, which binds iron in the gut to form insoluble iron oxalate that cannot be absorbed. The net calcium-available from spinach is approximately 5% — reflecting the severity of oxalate binding. Iron bioavailability from spinach is similarly impaired, making spinach a considerably less effective iron source than its total iron content implies.
Better choices in the dark leafy green category for iron bioavailability: kale (2.5mg per cup cooked, much lower oxalate than spinach — higher net bioavailability), Swiss chard (3.9mg per cup cooked, lower oxalate than spinach), and collard greens (2.1mg per cup cooked, low oxalate, high bioavailability). Broccoli provides 1mg per cup cooked with very low oxalate and provides its own vitamin C — making it a self-contained iron + absorption-enhancer combination.
Crucially, cooking all dark leafy greens significantly reduces oxalate content compared to eating them raw — boiling spinach and discarding the cooking water reduces oxalate by approximately 30–87%, improving iron bioavailability from the cooked preparation. For pregnancy, lightly cooked (not raw) leafy greens represent better iron delivery.
How to use it: Wilted kale with garlic and lemon in olive oil (low-oxalate iron source + vitamin C from lemon); Swiss chard sautéed with tomatoes and chickpeas; collard greens with black-eyed peas (a traditional Southern combination that is nutritionally well-calibrated for iron); broccoli stir-fried with lean beef and bell peppers (heme iron + meat factor + non-heme iron + vitamin C).
6. Blackstrap Molasses
Blackstrap molasses is the most concentrated non-heme iron source available from a non-animal whole food — a single tablespoon providing 3.5mg of iron in a form that many pregnant women find far more palatable and convenient than iron supplement tablets.
How it works: One tablespoon of blackstrap molasses (the dark, thick byproduct of sugar refining, not regular molasses) provides 3.5mg of iron, 200mg of calcium, and 200mg of potassium, alongside magnesium and some B vitamins. The iron in blackstrap molasses is non-heme iron, so absorption is enhanced by vitamin C and reduced by calcium (present in the molasses itself) and tannins — making the vitamin C pairing particularly important for this source.
The calcium content of blackstrap molasses is itself somewhat ironic — it provides iron alongside one of iron's primary absorption inhibitors. For maximum iron absorption from blackstrap molasses, consuming it in a morning oatmeal with orange juice or lemon water (vitamin C enhancement that can partially overcome the calcium competition) is more effective than consuming it with a glass of milk.
How to use it: One to two tablespoons stirred into warm oatmeal (the most practical daily delivery — the slightly bitter, mineral flavor blends well with oats), in smoothies with banana and orange juice, drizzled over yogurt, or dissolved in warm water with lemon and ginger as a mineral-rich morning tonic. Some women use it as a sweetener replacement in baking — ginger cookies, dark bread, marinades.
7. Pumpkin Seeds (Pepitas)
Pumpkin seeds are the most iron-dense seed available and simultaneously the best magnesium and zinc source from seeds — making them one of the most nutritionally comprehensive pregnancy snacks possible.
How it works: One ounce of pumpkin seeds provides 4.2mg of iron — the highest of any commonly consumed seed. The iron is non-heme, so absorption optimization through vitamin C pairing is important. The same ounce provides 156mg of magnesium (pregnancy requires 350mg daily, with deficiency associated with preeclampsia, preterm labor, and leg cramps) and 2.2mg of zinc (supporting the fetal immune system and neural tube development that zinc governs).
The tryptophan in pumpkin seeds (the highest of any seed) provides a dietary precursor for serotonin synthesis — relevant to the mood stabilization and sleep quality that pregnant women often struggle with and that adequate serotonin supports.
How to use it: One ounce as a daily snack with a vitamin C source (combine with dried apricots — which also provide non-heme iron — and a small orange, or add to a trail mix with dried mango); sprinkled over salads with tomatoes and lemon dressing; blended into smoothies; or used as a topping for overnight oats with berries.
8. Tofu (Firm, Calcium-Set)
Firm tofu is an excellent pregnancy iron source — particularly important for vegetarian and vegan pregnant women — providing non-heme iron alongside complete plant protein and calcium in a highly versatile culinary format.
How it works: Half a cup of firm tofu provides 3.4mg of iron alongside 8g of complete protein (all essential amino acids, rare among plant proteins) and the calcium that supports fetal bone development. The iron is non-heme and benefits significantly from vitamin C pairing — tofu stir-fried with bell peppers, tomatoes, or broccoli combines the iron source with its own absorption enhancer.
An important note on calcium-set tofu: the calcium sulfate used as a coagulant in most firm tofu is itself a mild iron absorption inhibitor — the same competition for DMT-1 absorption that affects dairy calcium applies here. For maximum iron absorption, pair tofu-based iron meals with vitamin C at the same time, and do not consume additional calcium-rich foods or drinks simultaneously.
Tofu's complete protein profile provides the amino acids essential for fetal tissue synthesis that plant protein sources with incomplete profiles (most legumes, grains) cannot provide alone — making tofu a particularly valuable pregnancy protein for plant-based eaters.
How to use it: Tofu scramble with spinach, bell peppers, and turmeric (iron + vitamin C + anti-inflammatory compounds); stir-fried firm tofu with broccoli and red bell pepper over brown rice (plant iron + high-vitamin C vegetables); tofu and edamame in miso soup with seaweed (multi-source plant protein and iron combination); marinated and baked tofu as a sandwich filling with tomato.
9. Dried Apricots and Dried Figs
Dried fruits — particularly dried apricots and dried figs — are the most iron-dense fruit sources available and represent a genuinely practical between-meal iron delivery strategy that requires no preparation.
How it works: Ten dried apricot halves (approximately 35g) provide 2.5mg of iron. Ten dried figs provide approximately 2mg of iron. Both are non-heme iron sources, and both provide significant potassium and fiber alongside their iron content — important for the constipation that iron supplements frequently cause and that pregnancy itself exacerbates through progesterone-mediated intestinal slowing.
Dried apricots additionally provide beta-carotene — a safe plant-derived vitamin A precursor (as opposed to the preformed retinol from liver that requires moderation in pregnancy). The fiber in dried fruits supports the gut microbiome that modulates iron absorption indirectly through gut barrier integrity and reduces the constipation that makes iron-rich meals uncomfortable.
Safety note: Sulfur dioxide is used as a preservative in many commercial dried apricots (giving them their vivid orange color). Unsulfured dried apricots are darker brown in color and preferred during pregnancy — sulfur dioxide has not been definitively established as safe for fetal exposure, and the sulfite hypersensitivity that affects approximately 1% of people is more concerning during pregnancy.
How to use it: A daily snack of 8–10 dried apricots with 2 tablespoons of pumpkin seeds and a vitamin C source (small orange, or combine with dried mango which also provides vitamin C and beta-carotene); added to overnight oats; in trail mix with nuts and dark chocolate (dark chocolate itself provides iron — approximately 3.3mg per oz of 70%+ dark chocolate); or served alongside a meal that contains a vitamin C-rich component.
10. Quinoa
Quinoa provides the most iron of any grain-like seed alongside a complete protein profile — making it the most nutritionally comprehensive iron-delivering carbohydrate base for pregnancy.
How it works: One cup of cooked quinoa provides 2.8mg of iron — significantly more than brown rice (0.8mg per cup cooked) or whole wheat pasta (3.3mg per cup, but higher in phytates). Quinoa's protein is complete — it contains all essential amino acids, unlike most grains — providing lysine that most plant proteins lack and that is particularly important for fetal tissue synthesis.
Quinoa's phytate content is meaningful but can be substantially reduced by rinsing raw quinoa thoroughly before cooking (removing the saponin coating that contains most of the phytate) and by soaking for 30 minutes to 2 hours before cooking. These simple preparation steps meaningfully improve iron bioavailability from quinoa.
How to use it: Quinoa breakfast bowl with berries (iron + vitamin C from berries) and pumpkin seeds (iron + magnesium + zinc); quinoa and black bean salad with lime juice and bell peppers (multiple iron sources + vitamin C from lime and peppers + folate from beans); quinoa stuffed bell peppers (the peppers themselves providing the vitamin C that enhances iron absorption from the quinoa and bean filling); or warm quinoa porridge with blackstrap molasses and dried apricots for a breakfast that stacks multiple iron sources simultaneously.
11. Dark Chocolate (70%+ Cacao)
Dark chocolate at 70% cacao or higher provides meaningful iron alongside flavanols with anti-inflammatory properties — and its palatability makes it one of the most sustainable daily iron contributors available.
How it works: One ounce (28g) of 70%+ dark chocolate provides 3.3mg of iron — a remarkable iron density from a food that most people eat as a treat rather than a nutritional strategy. The iron is non-heme, and absorption is somewhat inhibited by the tannins naturally present in cocoa — pairing with vitamin C (orange segments, strawberries) at the same time can partially offset this inhibition.
Dark chocolate's flavanols (epicatechin and catechin) have demonstrated anti-inflammatory effects through NF-kB inhibition — relevant to the inflammatory component of pregnancy complications including preeclampsia, which has an inflammatory pathogenesis. Observational studies have found associations between regular dark chocolate consumption during pregnancy and reduced preeclampsia risk, with the flavanol anti-inflammatory mechanism as the proposed explanation.
Magnesium (65mg per oz), zinc (0.9mg per oz), and copper (0.5mg per oz) in dark chocolate complement the iron for comprehensive mineral delivery.
Safety note: Limit to 1–2 ounces daily — dark chocolate's caffeine content (approximately 12mg per oz) is relevant to pregnancy caffeine limits (200mg daily maximum), and the theobromine content provides mild stimulant effects. High-quality 70–85% dark chocolate from ethical sourcing is preferred. Avoid during episodes of heartburn — chocolate relaxes the lower esophageal sphincter, exacerbating pregnancy reflux.
How to use it: One ounce of dark chocolate alongside a vitamin C source as an afternoon snack (orange + dark chocolate = iron + vitamin C absorption enhancement + satisfaction); dark chocolate stirred into morning oatmeal with blackstrap molasses and dried apricots for a mineral-dense breakfast; or as a topping for Greek yogurt with berries (though note that the calcium in yogurt will moderately compete with the dark chocolate iron — acceptable as part of a varied daily pattern, but best not to rely on this combination as a primary iron delivery strategy).
12. Sardines (Canned with Bones)
Sardines are the most nutritionally comprehensive pregnancy food available in a single can — providing heme iron, omega-3 DHA (critical for fetal brain and retinal development), vitamin D, calcium from edible bones, vitamin B12, and selenium in a combination that no other common food matches for pregnancy-specific nutritional importance.
How it works: A 3-ounce can of sardines provides 2.5mg of heme iron — absorbed at 15–35% efficiency — alongside 1,100mg of omega-3 DHA+EPA (critical for fetal brain development in the third trimester, when neuronal DHA incorporation is most rapid), 325mg of calcium (from edible bones — the same hydroxyapatite structure as human bone), and 245 IU of vitamin D. The DHA content of sardines is particularly important because breast milk DHA (important for infant brain development after birth) directly reflects maternal DHA intake during pregnancy.
Safety: Sardines are on the FDA/EPA "best choice" seafood list for pregnancy — a small fish with very low mercury accumulation, safe for consumption 2–3 times weekly. Canned sardines in water or olive oil; avoid sardines packed in brine or tomato sauce if sodium restriction is a concern.
How to use it: Sardines on whole grain rye crackers with avocado and lemon (heme iron + healthy fat for fat-soluble vitamin absorption + vitamin C from lemon); sardines in pasta with tomatoes and garlic (heme iron + vitamin C from tomatoes in a complete meal); sardines in a salad with leafy greens, tomatoes, and lemon dressing; or mashed sardine and avocado on toast — a genuinely nutritious and quick pregnancy lunch or dinner.
13. Edamame (Fresh Green Soybeans)
Edamame provides the highest protein-to-iron density of any fresh vegetable — combining non-heme iron with complete plant protein, folate, and the soy isoflavones that have demonstrated modest benefits for pregnancy outcomes in research.
How it works: One cup of cooked edamame provides 3.5mg of iron alongside 18g of complete protein — making it the most protein-dense plant iron source available. Folate from edamame (482mcg per cup — meeting the entire pregnancy folate recommendation in one serving) makes the iron + folate combination particularly valuable for first and second trimester consumption when folate demand for neural tube development is highest.
The oligosaccharides in edamame selectively feed Bifidobacterium gut bacteria — directly relevant to pregnancy because gut microbiome composition during pregnancy influences fetal immune programming, and the Bifidobacterium enrichment from fermented soy foods like miso and tempeh (closely related) has been specifically associated with reduced infant allergic disease risk.
How to use it: Edamame as a daily snack with a squeeze of lemon (iron + vitamin C in the simplest possible format); edamame in brown rice sushi bowls with ginger and pickled vegetables; edamame and quinoa salad with lime dressing and roasted bell peppers; or added to soups and stews for a protein and iron boost.
14. Fortified Breakfast Cereals (Low-Sugar, Whole Grain)
Whole grain, low-sugar fortified breakfast cereals are one of the few processed foods with a genuine pregnancy nutrition argument — many provide 100% of the daily iron requirement in a single serving with highly bioavailable ferric pyrophosphate or ferrous fumarate iron fortification.
How it works: Many fortified whole grain cereals (Total, Grape-Nuts, and specific Weetabix varieties) provide 18mg of iron per serving — the pre-pregnancy daily requirement in one bowl. The iron form used in fortification matters significantly: ferrous sulfate has good bioavailability; ferric pyrophosphate has lower bioavailability but fewer GI side effects; electrolytic iron (used in many cereals) has variable and often poor bioavailability. Check the label for iron form when possible.
The practical value of fortified cereal as a pregnancy iron source is highest when consumed with vitamin C (orange juice is the traditional companion — though whole orange is preferable for fiber retention) and without simultaneously consuming dairy (the calcium in milk competes with iron absorption). Consumed correctly, a bowl of high-iron fortified cereal with fresh orange juice provides an impressive morning iron delivery with minimal preparation.
Caution: High-sugar fortified cereals (most children's cereals, granolas with added sugar above 8g per serving) negate the iron benefit by triggering the glucose-driven inflammatory response that impairs iron absorption through oxidative stress. Low-sugar whole grain varieties only.
How to use it: As a pregnancy emergency iron source when cooking is not possible — one bowl of Total or Grape-Nuts with orange juice provides more iron than most carefully prepared homemade meals. Not a substitute for diverse whole-food iron sources, but a practical backup.
15. Hemp Seeds and Sunflower Seeds
Hemp seeds round out the seed category with a distinctive nutritional profile that complements pumpkin seeds — providing meaningful non-heme iron alongside the ideal omega-6:omega-3 ratio that supports fetal anti-inflammatory development.
How it works: Three tablespoons of hemp seeds provide 2.4mg of iron alongside 10g of complete protein, the essential fatty acids ALA omega-3 and gamma-linolenic acid (GLA) in a 3:1 omega-6:omega-3 ratio (considered optimal for anti-inflammatory fatty acid metabolism), magnesium, and zinc. The complete protein content of hemp seeds — rare among plant sources — provides all essential amino acids for fetal tissue synthesis without requiring protein complementation.
Sunflower seeds provide 2.5mg of iron per ounce alongside 8.6mg of vitamin E per ounce — the highest vitamin E content of any seed, relevant to pregnancy because vitamin E is a critical antioxidant protecting against the oxidative stress of pregnancy and supporting placental function. Sunflower seeds provide selenium (important for thyroid function during pregnancy — thyroid hormone changes are profound in pregnancy and selenium deficiency is associated with hypothyroidism) at 32mcg per ounce.
How to use it: Three tablespoons of hemp seeds stirred into overnight oats or smoothies (the neutral flavor makes them imperceptible in most preparations); sunflower seed butter (equivalent to peanut butter in protein and nutritionally superior in vitamin E and selenium) on whole grain toast with sliced strawberries (iron + vitamin E + vitamin C absorption enhancement); mixed seed trail mix with pumpkin seeds, hemp seeds, and dried apricots as a comprehensive pregnancy iron snack.
Iron Absorption Maximizers and Blockers
The Top 5 Strategies to Maximize Iron Absorption
1. Vitamin C at every iron-rich meal: Fifty to 100mg of vitamin C (half a lemon, a small orange, half a red bell pepper, or a cup of strawberries) at the same meal as iron-rich foods dramatically improves non-heme iron absorption. Vitamin C reduces ferric iron (Fe³⁺) to ferrous iron (Fe²⁺), the absorbable form, and forms soluble iron-ascorbate complexes that resist the inhibitory effects of phytates and oxalates. The improvement in non-heme iron absorption from vitamin C co-consumption ranges from 2-fold to 6-fold depending on the meal's initial iron bioavailability. This single strategy is the highest-leverage iron optimization available and should be applied at every plant-iron-containing meal.
2. Pair non-heme iron with small amounts of heme iron: The meat factor — the enhancement of non-heme iron absorption produced by simultaneously consuming even a small amount of heme iron — can increase plant iron absorption by 50–150%. A small amount of beef, chicken, or fish alongside a legume or vegetable iron source meaningfully improves total meal iron absorption. Even 30g (1 oz) of meat alongside a predominantly plant-based meal produces measurable enhancement of non-heme iron bioavailability.
3. Time iron-rich meals away from tea, coffee, and dairy: Tannins in tea and coffee form insoluble complexes with iron in the gut, reducing absorption by 50–70% when consumed simultaneously. Calcium from dairy products directly competes with iron for DMT-1 absorption. The practical recommendation: consume tea and coffee at least 1–2 hours away from iron-rich meals, and do not have a glass of milk alongside an iron-focused meal. Herbal teas (peppermint, ginger, chamomile) do not contain iron-inhibiting tannins and are safe to consume alongside iron-rich meals.
4. Cook in cast iron: Acidic foods cooked in seasoned cast iron cookware absorb measurable amounts of iron from the cooking surface. Tomato sauce simmered for 20 minutes in cast iron can absorb 5–7mg of iron per serving. Scrambled eggs cooked in cast iron gain approximately 2.5mg per serving. This "accidental" iron fortification represents a meaningful daily contribution to iron intake with zero dietary effort.
5. Soak, sprout, and ferment legumes and grains: Phytates — found in legumes, whole grains, and seeds — bind non-heme iron in the gut and significantly reduce absorption. Soaking dried legumes for 12–24 hours before cooking (and discarding the soaking water) reduces phytate by 30–50%. Sprouting reduces phytate by 50–75%. Fermentation (sourdough bread, fermented soy) reduces phytate to near-zero levels. These preparation methods can improve non-heme iron bioavailability from legumes and grains by 2-fold or more.
The Top 5 Iron Absorption Blockers to Avoid
Calcium at the same meal: Calcium competes directly with iron for DMT-1 intestinal absorption. Dairy products, calcium-fortified plant milks, and calcium supplements consumed at the same time as iron-rich foods significantly reduce absorption. Space calcium consumption by at least 1–2 hours from iron-rich meals.
Tea and coffee: Polyphenols and tannins in tea reduce iron absorption by 50–90% when consumed with or immediately after an iron-rich meal. Even one cup of tea consumed with a meal can negate a meaningful portion of the iron available from that meal. This is one of the most commonly underappreciated sources of iron deficiency in otherwise iron-conscious pregnant women who habitually drink tea with meals.
High-phytate foods without preparation strategies: Unsoaked whole grains and legumes consumed alongside iron-rich foods without vitamin C co-consumption can dramatically reduce the iron available from the meal. Prepare legumes properly (soak, discard soaking water) and pair all high-phytate iron meals with vitamin C.
Zinc and calcium supplements taken simultaneously with iron supplements: High-dose zinc and calcium supplements compete with iron for DMT-1 absorption. If taking both iron and calcium supplements (common in pregnancy), space them by at least 2 hours. Iron and prenatal zinc supplements can be taken together as the doses in prenatals are balanced.
Antacids containing calcium carbonate: Many pregnancy-safe antacids (Tums) contain calcium carbonate, which will bind iron if taken simultaneously with iron-rich meals or iron supplements. Take antacids at least 2 hours away from iron supplement doses.
A Day of Iron-Rich Eating in Pregnancy
Sample High-Iron Pregnancy Day
Breakfast (approximately 12–15mg iron):
Half cup rolled oats with 1 tbsp blackstrap molasses, 2 tbsp pumpkin seeds, 1 cup mixed berries, and a tablespoon of ground flaxseed
One cup of orange juice or a whole orange (vitamin C for iron absorption)
Herbal tea (not black or green tea — avoid tannins at breakfast)
Iron sources: oats, molasses, pumpkin seeds, flaxseed | Absorption enhancers: berries (vitamin C), orange
Mid-morning snack (approximately 4–5mg iron):
10 dried apricots with 1 oz dark chocolate (70%+)
Small glass of lemon water
Iron sources: dried apricots, dark chocolate | Absorption enhancer: lemon vitamin C
Lunch (approximately 8–10mg iron):
Lentil and chickpea soup with tomatoes, spinach, and lemon
Whole grain rye bread
Side of raw red bell pepper slices
Water or herbal tea
Iron sources: lentils, chickpeas, spinach | Absorption enhancers: tomatoes, lemon, red bell pepper (all very high vitamin C)
Afternoon snack (approximately 2–3mg iron):
Edamame with sea salt and lemon squeeze
Iron source: edamame | Absorption enhancer: lemon
Dinner (approximately 8–10mg iron):
Lean grass-fed beef (3oz) stir-fry with broccoli, red bell peppers, bok choy over quinoa
Green salad with lemon-olive oil dressing
Water with lemon
Iron sources: beef (heme), broccoli, bok choy, quinoa | Absorption enhancers: bell pepper, broccoli (its own vitamin C), lemon | Meat factor from beef enhancing non-heme iron absorption from all vegetables
Estimated total daily iron from food: 35–40mg (significantly above the 27mg pregnancy target, accounting for absorption variability that will bring actual absorbed iron to approximately 8–15mg — within the 27mg intake target range when bioavailability is factored in)
Frequently Asked Questions
Do I need an iron supplement in addition to eating iron-rich foods?
Most pregnant women benefit from iron supplementation in addition to dietary iron optimization — because the 27mg daily requirement is genuinely difficult to meet through food alone, particularly in the second and third trimesters when demands are highest. The standard prenatal vitamin provides 27mg of supplemental iron (ferrous sulfate, ferrous fumarate, or ferrous gluconate — all acceptable forms), which combined with dietary iron should cover most women's needs.
Iron supplementation is specifically indicated if your third-trimester blood panel shows hemoglobin below 11g/dL (anemia) or serum ferritin below 30ng/mL (depleted iron stores even without anemia). Discuss your specific needs with your obstetrician or midwife — some women with strong dietary iron intake from diverse heme and non-heme sources and good absorption strategies may not require high-dose supplemental iron, while others with plant-exclusive diets, prior anemia, or multiple pregnancies may require higher supplementation.
Iron supplements are best absorbed when taken on an empty stomach or with vitamin C, without calcium supplements, dairy, or tea. If iron supplements cause nausea (a common side effect), take with a small amount of food — absorption is slightly reduced but significantly less nausea.
Is it safe to eat fish during pregnancy for iron?
Most fish is safe and strongly encouraged during pregnancy — the omega-3 DHA from fatty fish is one of the most important pregnancy nutrients for fetal brain development, and fish provides heme iron with good bioavailability. The FDA and EPA recommend 8–12 ounces (2–3 servings) of low-mercury fish weekly during pregnancy, specifically including: sardines, salmon, trout, herring, anchovies, and canned light tuna (not albacore/white tuna, which is higher in mercury). Avoid: swordfish, king mackerel, tilefish, bigeye tuna, orange roughy, marlin, and shark — all high-mercury species contraindicated in pregnancy.
What are the symptoms of iron deficiency anemia in pregnancy?
The classic symptoms of iron deficiency anemia in pregnancy include: persistent fatigue and weakness beyond normal pregnancy tiredness, pallor (pale gums, inner eyelids, and nail beds), shortness of breath with minimal exertion, heart palpitations, dizziness or lightheadedness (particularly on standing), cold hands and feet, and headaches. A particularly specific symptom of iron deficiency is pica — cravings for non-food substances including ice (pagophagia), clay, dirt, or starch. If you develop pica during pregnancy, discuss it with your healthcare provider immediately as it is a reliable indicator of significant iron deficiency. Regular blood panels (typically at the first prenatal visit and again at 24–28 weeks) can identify deficiency before symptoms develop.
Can I get too much iron from food during pregnancy?
Iron toxicity from food sources alone is extremely rare in pregnancy — the intestine tightly regulates iron absorption and downregulates it when iron stores are adequate through the hormone hepcidin. The concern about excess iron applies primarily to supplemental iron at very high doses (above 45mg elemental iron daily beyond prenatal supplementation) and to individuals with hereditary hemochromatosis (a genetic condition causing unregulated iron absorption — if you have a family history of hemochromatosis, discuss iron management with your doctor before pregnancy and during it). Do not exceed supplemental iron doses without medical guidance.
How does morning sickness affect iron intake?
First-trimester nausea and vomiting — affecting 70–80% of pregnant women — can make iron-rich foods difficult to tolerate during the period when establishing good iron nutrition habits is most important. Several practical strategies: iron supplements are often better tolerated later in the day after nausea has subsided; liquid iron supplements (like Floradix or Spatone) tend to cause less nausea than ferrous sulfate tablets; taking iron with a small amount of carbohydrate rather than on an empty stomach reduces nausea; dried apricots and dark chocolate tend to be more tolerable iron sources during nausea periods than strong-smelling red meat or leafy greens; and cold foods generally produce less nausea than hot foods — cold smoothies containing spinach, berries, and citrus can deliver meaningful iron during nausea episodes when hot meals are impossible.
References and Further Reading
Bothwell TH — American Journal of Clinical Nutrition (2000) — Iron requirements in pregnancy and strategies to meet them Foundational review establishing the physiological basis for the 27mg daily iron requirement in pregnancy — including the detailed quantification of iron needed for red blood cell expansion (450mg), fetal accumulation (270–300mg), placental development (50mg), and delivery blood loss coverage, with the trimester-by-trimester demand profile confirmed through isotopic studies.
Georgieff MK — American Journal of Clinical Nutrition (2007) — Iron deficiency in pregnancy: fetal and neonatal neurodevelopmental consequences Comprehensive review of the neurodevelopmental consequences of gestational iron deficiency — hippocampal vulnerability, dopaminergic system impairment, myelination deficits, and the long-lasting cognitive and behavioral consequences that may not manifest until school age — establishing the developmental case for aggressive gestational iron management beyond maternal anemia prevention.
Hurrell R & Egli I — American Journal of Clinical Nutrition (2010) — Iron bioavailability and dietary reference values Definitive review of heme vs. non-heme iron bioavailability, absorption enhancers (vitamin C, meat factor), inhibitors (phytates, tannins, calcium), and the mathematical modeling used to establish dietary iron reference values — the most rigorous available evidence base for the practical dietary strategies described in this guide.
WHO Global Anaemia Estimates (2021) — Prevalence of anaemia in women of reproductive age World Health Organization global data confirming that anaemia affects 37% of pregnant women worldwide, with iron deficiency as the primary cause in approximately 50% of cases — establishing gestational iron deficiency as the most widespread nutritional emergency in maternal health globally, disproportionately affecting women in low-income countries and those with multiple pregnancies.
About the Author
I'm Judith, a wellness enthusiast and Applied Bio Sciences and Biotechnology graduate behind BiteBrightly. With a deep-rooted belief in the healing power of food, my nutrition journey began with a personal transformation—I improved my eyesight through targeted dietary changes. This life-changing experience sparked my mission to empower others by sharing evidence-based insights into food as medicine.
Drawing on my scientific background, personal experience, and ongoing research into nutrition and health, I focus on breaking down complex health topics into clear, practical, and actionable guidance. My approach combines scientific credibility with real-world application, making evidence-based nutrition accessible to everyone.
Follow me on Pinterest for daily health tips, recipes, and wellness inspiration.
Important Notice: The information in this article is for educational purposes only and is not intended as medical advice. I am not a medical doctor, registered dietitian, midwife, or obstetrician. Iron requirements, supplementation needs, and dietary recommendations during pregnancy are individual and should be discussed with your qualified healthcare provider — particularly if you have a history of iron deficiency anemia, hemochromatosis, inflammatory bowel disease, or other conditions affecting iron metabolism. All supplementation during pregnancy should be discussed with your obstetrician or midwife before beginning. The vitamin A content of liver is a genuine teratogenic concern at excess doses — follow the frequency guidelines in this article and discuss liver consumption with your healthcare provider. Seafood safety guidance follows current FDA/EPA recommendations for pregnancy but should be verified with your healthcare provider for your specific circumstances. These statements have not been evaluated by the FDA.
Connect
Join our newsletter for fresh health tips
© 2026. All rights reserved.